
As health systems continue to slowly transition to Alternative Payment Models (APM), they are faced with an immense challenge – how to expand their footprint in risk-based arrangements given the highly variable levels of revenue at play.
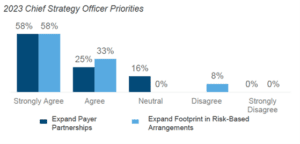
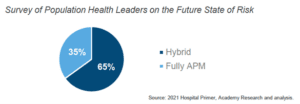
In fact, within The Academy’s Leading Health Systems (LHS), the majority of health system revenue is still tied to Fee-For-Service (FFS) payment. However, going into 2023, Chief Strategy Officers remain committed to increasing financial risk through value-based arrangements. As a result, the end state is expected to be a “foot in two boats,” with 65% of Population Health Leaders expecting a hybrid FFS + APM model.
The Many Flavors of Alternative Payment Models
When considering how to market towards health systems as it relates to alternative payment models, it’s important to remember that it’s not a “one size fits all” approach. There are many flavors of alternative payment models:
- Pay for Performance: Paid traditional fee-for-service model but can earn bonuses or receive penalties based on performance on quality and other metrics
- Examples: Quality Payment Program, Hospital Readmissions, Reduction Program
- Bundled Payments: Paid a lump sum for all services related to a procedure over a defined period; incentivized to reduce cost, but not to reduce volumes
- Examples: Comprehensive Care for Joint Replacement, Maternity bundled payments
- Shared Risk: Often paid FFS over course of year but total cost compared against benchmark at year-end; can earn savings or owe payer money for overspending
- Examples: Medicare Shared Savings Program, Commercial ACOs
- Capitation: Paid a fixed amount per patient regardless of what services are provided; typically thought of as high risk, high reward
- Examples: Medicare Direct Contracting, some Medicare Advantage
Strategies to Align Your Pitch to Health Systems’ Value-Based Care Goals
Industry innovators have an opportunity to better articulate the ways in which they can support Leading Health Systems during this transition.
Here are strategies that were discussed in the webinar:
- Be specific when using terms like cost reduction. Who are you reducing costs for? (i.e., the patient, the health system, the payer).
- Ensure that you’re familiar with the factors that influence adoption of value-based payment, such as:
- Payer interest
- Leading HS strategic priorities
- State-wide initiatives
- Competitor adoption of value-based contracts
- Market capture
- Owned health plan
- Mandatory government payer programs
- Make sure that you’re familiar with the three archetypes of health system risk portfolios. Their 2023 areas of focus and incentive to expand VBC footprint will depend on their degree of risk, as well as external factors like population demographics and market capture.
- FFS Holdouts
- VBC-focused Adopters
- VBC-focused Innovators
- Articulate the urgency and quantify the downstream negative consequences of the problem your solution solves
- Develop a strong case for the differentiation of your solution and why it is the best way to solve that problem (vs competitor or status quo)
- Emphasize the positive near-term financial impact of partnering (i.e., amount of input cost savings, financial impact of increased patient access)
For more specifics on how to align your pitch and implement the strategies above, access the webinar recording.