What 70 Million Medicaid Recipients Don't Know About Their Coverage
Published 6/4/2026, Updated 7/14/2026
Author: Andrew Reed, Assoc. Director, The Health Management Academy
Survey Findings on Awareness, Behavioral Intent, and Access Among Medicaid Enrollees Ahead of 2027 Eligibility Changes
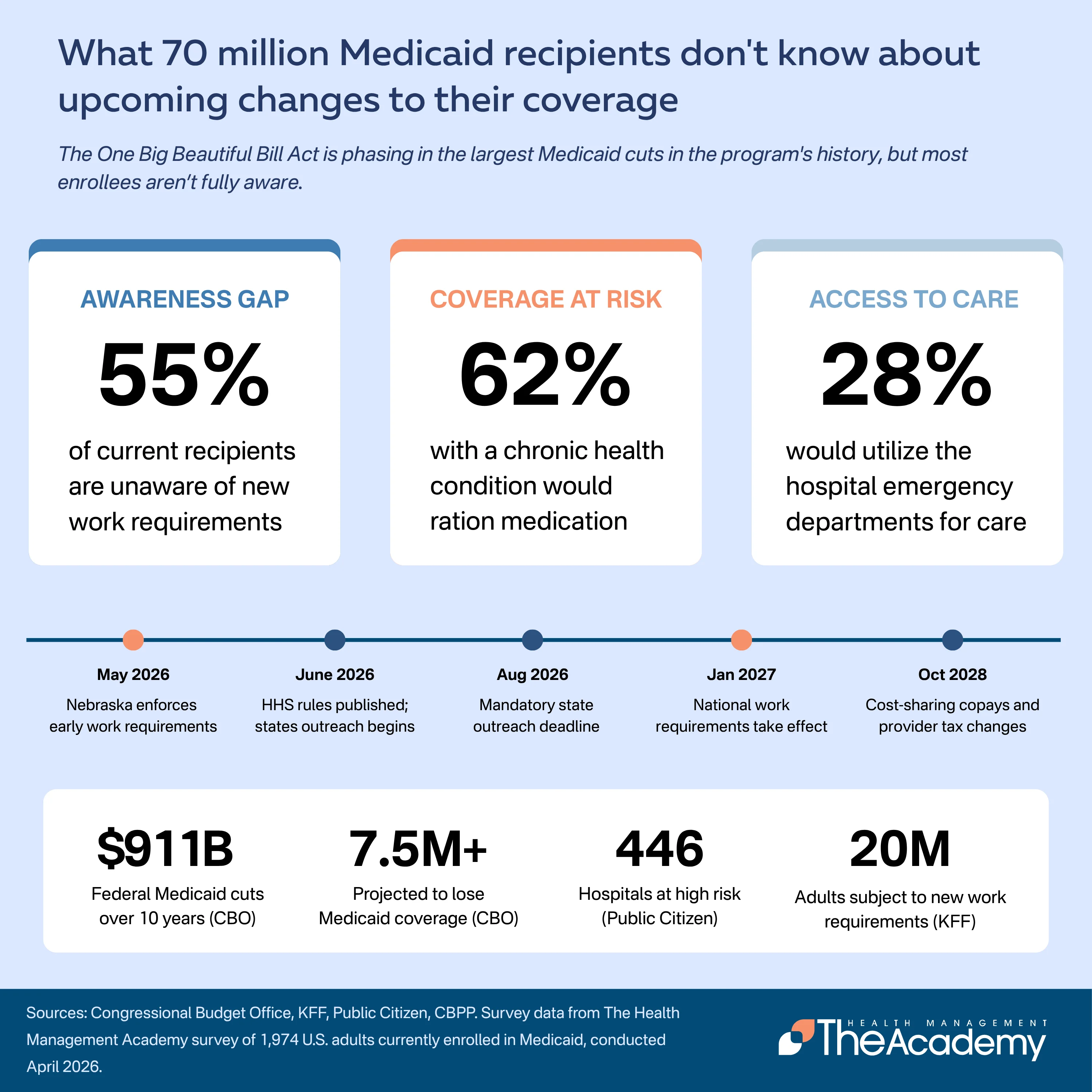
The One Big Beautiful Bill Act, signed into law on July 4, 2025, enacted the largest reduction in federal Medicaid spending in the program's history. The Congressional Budget Office estimates the law will reduce federal Medicaid spending by $911 billion over a decade and increase the number of uninsured Americans by 7.5 million or more. Among the most consequential provisions are new work requirements for adults ages 19 to 64 enrolled in Medicaid through the ACA expansion, effective January 1, 2027, and a shift from annual to semiannual eligibility redeterminations. States must begin enrollee outreach no later than June 30, 2026, and the Department of Health and Human Services is required to issue an interim final rule on implementation by June 2026.
Policymakers, state Medicaid agencies, and health policy researchers have studied the legislation extensively since its passage. However, there has been limited information about what the people most directly affected by these changes know, what they expect, and what they say they would do if they lost coverage. To address this gap, The Health Management Academy surveyed 1,974 adults currently enrolled in Medicaid in April 2026 to assess awareness of the coming eligibility changes, anticipated behavioral responses to potential coverage loss, and current access to care. This brief presents the survey's key findings, organized around three themes: the gap between what enrollees know and what is coming, the actions enrollees say they would take if coverage were lost, and the barriers enrollees face in accessing care if their nearest hospital closed or reduced services.
Key Findings
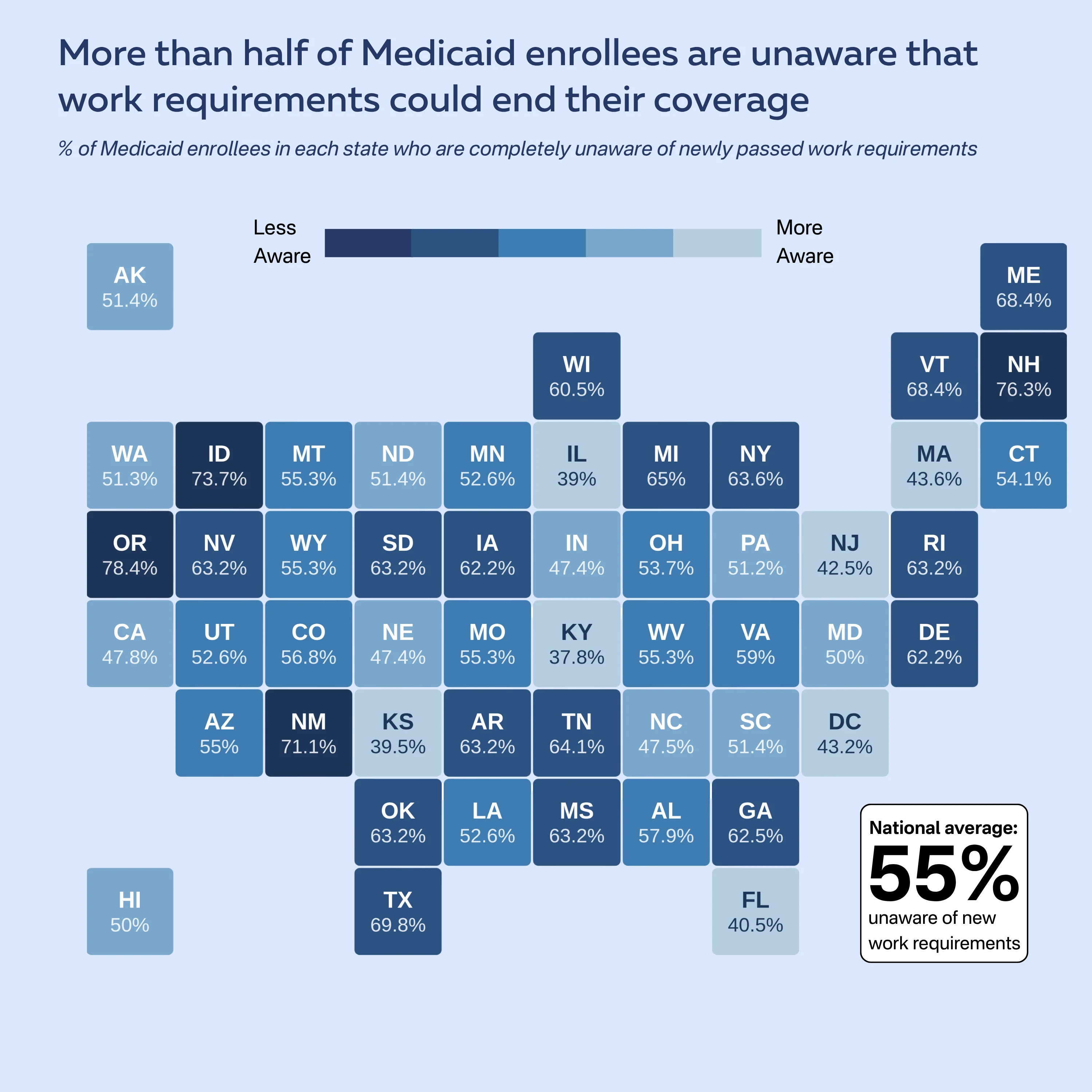
About 55% of Medicaid enrollees are completely unaware that work requirements will become a condition of eligibility starting January 2027. An additional 27% say they have heard something but are unsure of the details.
Roughly 85% of enrollees do not know that eligibility redeterminations will shift from annually to every six months.
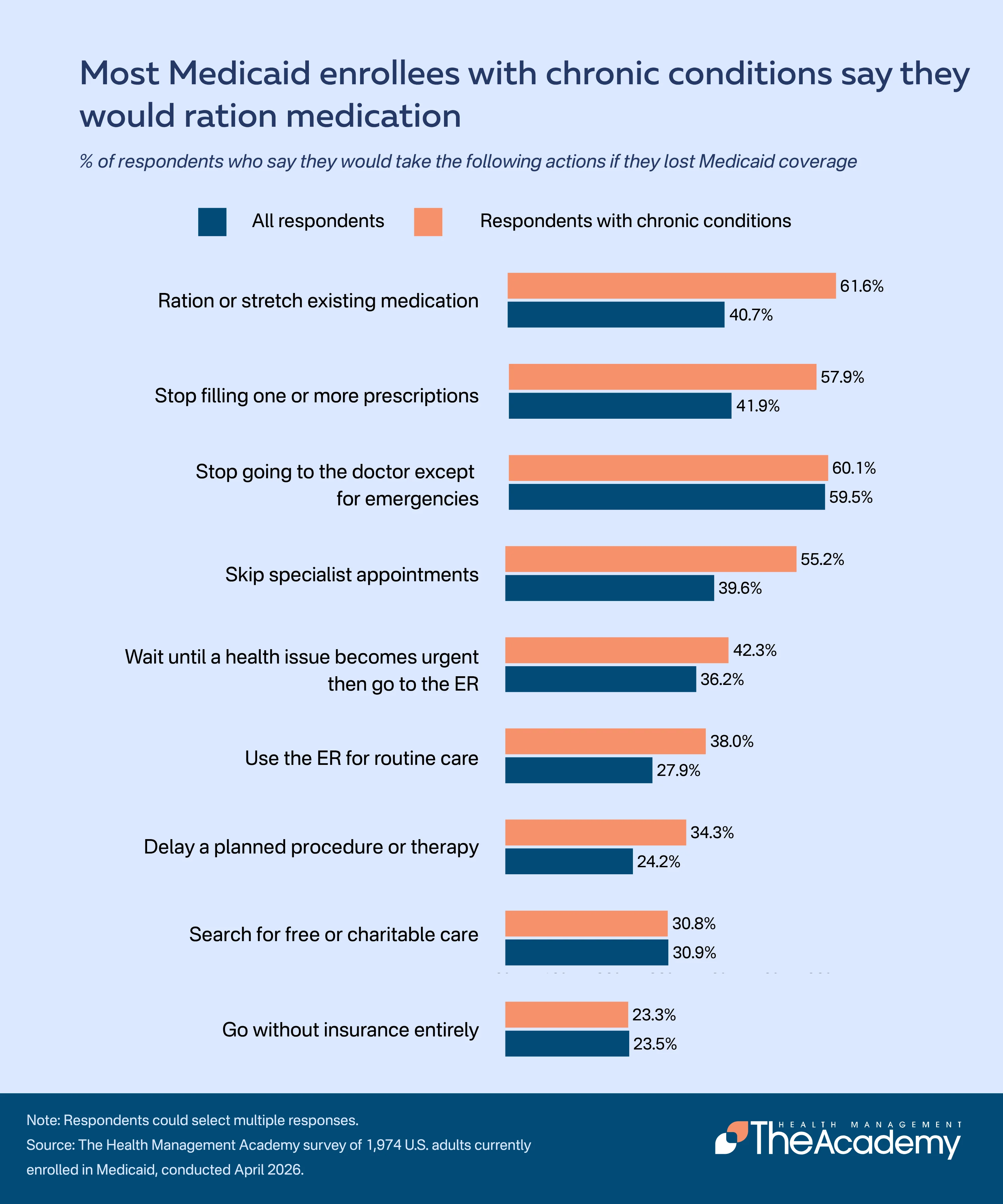
Among enrollees with chronic conditions, about 62% say they would ration their medication and 58% say they would stop filling at least one prescription, with significant overlap between the two groups.
Mental health medications are the most commonly identified category that enrollees say they would stop taking first (25%), followed by blood pressure and cholesterol medications (22%) and diabetes medications (17%).
About 37% of all respondents say they would wait until a health issue became urgent and then go to the emergency room. An additional 28% say they would use the emergency room for routine care.
Among enrollees with chronic conditions, nearly two-thirds say they would turn to the emergency room if they lost coverage.
Roughly 62% of enrollees do not drive themselves to medical appointments, and 42% say they could not travel farther than they currently do if their nearest hospital closed.
Black enrollees reported the highest rate of unawareness of work requirements (62%) and were the most likely to say they could not travel farther if their nearest hospital closed (44%), consistent with Public Citizen's finding that at-risk hospitals disproportionately serve Black and Hispanic communities.
Most Medicaid Enrollees Have Heard Little or Nothing About Coming Eligibility Changes
The April 2026 poll asked enrollees how much they had heard about recent changes to Medicaid eligibility. Nearly half (48%) said they had heard "nothing at all", and an additional 32% said they had heard only "a little". About 20% said they had heard "some" or "a lot".
When asked specifically about work requirements, 55% of enrollees said they were not aware that completing 80 hours per month of work, job training, education, or community service would become a condition of Medicaid eligibility in January 2027. About 27% said they had heard something but were unsure of the details. Only 17% said they were aware. Awareness of the shift to semiannual eligibility redeterminations was even lower: 85% of respondents said they did not know.
These findings are similar to those collected in Arkansas, where the state implemented Medicaid work requirements in 2018. A Harvard telephone survey of low-income adults conducted after that policy was in effect found that more than 70% of Arkansans subject to the requirement were unsure whether the policy was in place, despite extensive state outreach efforts including nearly 600,000 letters, 230,000 phone calls, and hundreds of social media posts.
Awareness levels varied across states. Among the states with the largest Medicaid enrollment, enrollees in Oregon (78%), Texas (70%), Georgia (63%), and Wisconsin (61%) reported the highest rates of being completely unaware of work requirements. Nebraska, the only state that has begun enforcing work requirements ahead of the federal deadline, showed a lower rate (48%), though nearly half of enrollees there remain unaware.
Despite this low awareness, about one-third (33%) of enrollees said they believe they will "definitely" still be eligible for Medicaid in January 2027. An additional 32% said "probably yes". Only 13% said "probably not" or "definitely not". The remainder (22%) said they were not sure, a finding that aligns with the overall pattern of limited information reaching this population ahead of the outreach window.
Enrollees with Chronic Conditions Say They Would Ration Medication and Delay Care
Respondents were also asked which, if any, actions they would take if they lost their Medicaid coverage. The most commonly selected response was stopping routine doctor visits unless a situation became an emergency (60%). About 41% said they would ration or stretch their existing medication, and a similar share said they would stop filling at least one prescription, with considerable overlap between the two responses. Nearly 40% said they would skip specialist appointments, and 24% said they would delay a planned procedure or surgery. About 23% said they would go without insurance entirely.
These rates were substantially higher among the 49% of respondents who reported having a chronic health condition requiring ongoing medication or treatment. Among this group, 6 in 10 said they would ration medication and 58% said they would stop filling at least one prescription, with significant overlap between the two responses. About 55% said they would likely skip specialist appointments. In each case, the rates among enrollees with chronic conditions exceeded those of the overall population by 15 to 20 percentage points.
A recent precedent illustrates what happens when Medicaid enrollees face administrative hurdles at scale. When pandemic-era protections that had kept people continuously enrolled in Medicaid expired in 2023, states rechecked eligibility for all enrollees in a process known as the "unwinding". More than 25 million people were disenrolled, and roughly 70% lost coverage because of paperwork problems rather than actual ineligibility.
The Harvard study of Arkansas's work requirements found that among those who lost coverage, 64% delayed taking medications because of cost, and 56% delayed care because of cost. A KFF survey of adults disenrolled during the Medicaid unwinding found that 56% skipped or delayed care or prescriptions while attempting to renew coverage. The survey data presented here capture behavioral intent rather than observed behavior, but the consistency with prior real-world outcomes suggests the responses reflect realistic expectations.
Mental Health Medications Are the Prescriptions Most Likely to Be Discontinued First
Among respondents currently taking one or more prescription medications, 25% identified mental health medications as the category they would stop taking first if they could no longer afford their prescriptions. Blood pressure and cholesterol medications were the second most common response (22%), followed by diabetes medications (17%), pain medications (16%), and respiratory medications (10%).
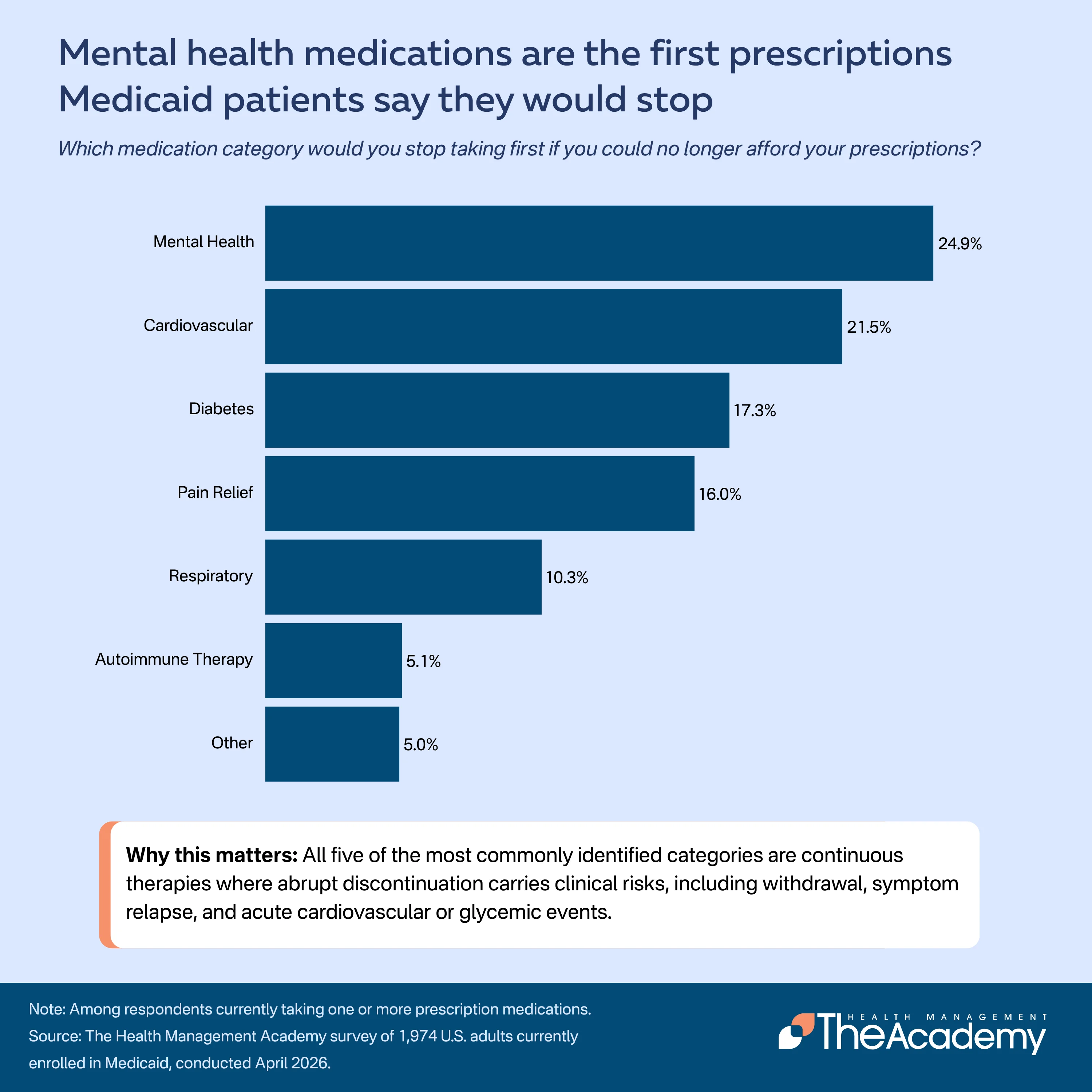
The concentration of risk in mental health, cardiovascular, and diabetes medications is notable because all three are continuous therapies where interruption carries clinical consequences. Abrupt discontinuation of antidepressants and anxiolytics carries risks of withdrawal and symptom relapse. Interruption of antihypertensives and statins is associated with elevated cardiovascular risk that compounds over time. Discontinuation of diabetes medications can lead to acute glycemic events.
For pharmaceutical manufacturers and health plans, these data points represent an early signal of adherence disruption across large chronic-disease populations. Coverage changes may not appear in claims data for several months after the work requirement deadline, but the behavioral intent measured here provides visibility into which therapeutic categories are most exposed. For organizations managing adherence programs or patient support services, this means that mental health, cardiovascular, and diabetes therapies should be prioritized for proactive intervention planning ahead of January 2027. Enrollees who anticipate losing coverage are identifying specific medications they would discontinue, which gives manufacturers and health plans a window to design targeted support, whether through patient assistance programs, copay mitigation strategies, or bridge coverage pathways, before disruption begins. Commercial forecasting models that rely on historical claims patterns may not capture the speed or concentration of the coverage shift that work requirements are expected to produce, particularly in expansion states where chronic-disease populations are largest.
Majority of Enrollees Would Turn to Emergency Departments if Coverage Were Lost
Two survey items captured different dimensions of emergency department utilization following coverage loss. About 37% of respondents said they would wait until a health issue became urgent and then go to the emergency room. Roughly 28% said they would use the emergency room for routine care they currently receive from a regular doctor. Among respondents with chronic conditions, nearly two-thirds said they would turn to the emergency room in at least one of these ways.
Hospital capacity is shrinking at the same time that ER demand is poised to grow. An April 2026 analysis by Public Citizen identified 446 hospitals across 44 states and Washington, D.C., at high risk of closing or reducing services as a result of the Medicaid funding cuts. These hospitals derive at least 20% of their revenue from Medicaid and related programs and have been operating at a loss. The analysis found that 60% of the at-risk facilities are in urban areas, and that the communities they serve have larger shares of Black and Hispanic residents and higher rates of poverty than communities served by other hospitals.
The convergence of these two data points, increased emergency department utilization among enrollees losing coverage and reduced capacity among the hospitals most likely to absorb that utilization, represents a compounding risk for health systems already operating under financial strain.
Many Enrollees Face Significant Barriers to Reaching Care if Hospitals Close
When asked how they normally travel for medical care and whether they could travel farther if their nearest hospital closed or reduced services, about 62% of respondents said they do not drive themselves to medical appointments. Among this group, 27% rely on a family member or friend for transportation, 22% use public transit, and 12% walk or use other means.
About 42% of all respondents said they could not travel any farther than they currently do if their nearest hospital closed. Among respondents with chronic conditions, 25% said a hospital closure would make managing their condition "much harder".
These access barriers were more pronounced among rural respondents, who reported greater distances to their nearest hospital and fewer transportation options. The $50 billion Rural Health Transformation Fund included in the reconciliation law is intended to support rural health infrastructure, but the Congressional Budget Office has projected that federal Medicaid spending in rural areas will decline by substantially more than the fund provides.
The data also shines light on disparities across racial and demographic groups. Black enrollees reported the highest rate of unawareness of work requirements (62%), compared to 56% among White enrollees and 54% among Hispanic enrollees. Black enrollees were also the most likely to say they could not travel farther if their nearest hospital closed (44%). These findings align with the Public Citizen analysis, which found that at-risk hospitals serve communities with larger shares of Black and Hispanic residents and higher rates of poverty than communities served by other hospitals.
Older enrollees (ages 55 and older) were less aware of the coming changes than younger adults and more likely to say they would ration medication, with 47% of those 65 and older selecting that response compared to 35% of those ages 25 to 34. In urban areas, 73% of enrollees said they do not drive themselves to medical appointments and 45% said they could not travel farther, reflecting high dependence on public transit systems that may not connect to alternative facilities if nearby hospitals close.
What's at Stake
The federal implementation timeline for Medicaid eligibility changes is compressed. The HHS interim final rule on work requirements was published June 1, 2026. States must begin enrollee outreach no later than June 30, 2026 and complete initial outreach by August 31, 2026. The national work requirement deadline is January 1, 2027, though the Secretary of HHS may grant good-faith extensions through December 31, 2028. Cost-sharing requirements and provider tax changes will phase in through October 2028.
The Health Management Academy's survey findings indicate that when outreach begins this summer, it will reach a population that is largely starting from a baseline of no information. The awareness gap measured here is not a reflection of enrollees hearing the message and choosing to disregard it. In most states, the message has not yet been delivered. The behavioral responses enrollees describe, rationing medication, discontinuing prescriptions, and shifting to emergency care, are consistent with what prior research has documented in Arkansas and during the Medicaid unwinding when coverage was disrupted. The difference is the scale at which these changes are now being implemented. For health systems, the operational implications are immediate. The same Medicaid populations that generate consistent inpatient and outpatient volume are the ones most likely to delay care, ration medication, and shift to emergency departments if coverage is disrupted. Systems with significant Medicaid payer mix face a direct revenue impact: fewer covered visits, more uncompensated emergency care, and higher acuity when patients present after months of deferred treatment. The 446 hospitals identified as at-risk employ 275,000 direct care workers, and facilities that close or cut services will push patients to neighboring systems that may already be operating near capacity. Health systems in expansion states should be modeling the volume and revenue impact of work requirement implementation now, using their own payer mix data alongside the enrollment and coverage loss projections published by KFF and CBO, rather than waiting for the effects to appear in quarterly results.
Methodology
This survey was conducted by The Health Management Academy in April 2026. A total of 1,974 U.S. adults currently enrolled in Medicaid were surveyed nationally. The sample was weighted to reflect Medicaid population demographics by age, race and ethnicity, income, geographic setting (urban, suburban, and rural), and state of residence. Survey questions assessed awareness of Medicaid eligibility changes enacted under the One Big Beautiful Bill Act (H.R. 1), anticipated behavioral responses to potential coverage loss, current prescription medication use, transportation to medical care, and proximity to hospital services.
Hospital risk data referenced in this brief is drawn from Public Citizen's April 2026 analysis of hospital financial data from the Centers for Medicare and Medicaid Services (2022 to 2024). Federal funding reduction estimates are based on KFF's allocation of Congressional Budget Office projections across the states. Medicaid enrollment data is from the KFF Medicaid Enrollment and Unwinding Tracker. Arkansas work requirement outcomes are from Sommers et al., "Medicaid Work Requirements in Arkansas: Two-Year Impacts on Coverage, Employment, and Affordability of Care," Health Affairs, September 2020.